

Knee osteoarthritis is a chronic joint disease characterized by the progressive softening of the articular cartilage, leading to the loss of its normal hardness. This process is accompanied by the formation of new bone and cartilage at the margins of the knee (osteophytes) as well as thickening and contraction of the joint capsule.
Although it is primarily a condition of older adults, knee osteoarthritis can also develop in younger patients if the cartilage is injured or subjected to abnormal loading over time. It is more common in women after menopause and in overweight patients.
Pain is the main symptom. In the early stages, it subsides with rest, but over time, remission is incomplete. As the disease progresses, nocturnal pain may occur, making it difficult for the patient to find a comfortable position.
Stiffness is another frequent symptom and tends to worsen over time.
Joint swelling (hydrarthrosis or synovitis) is common.
Deformity and disturbance of the joint axis also frequently occur, often associated with knee instability and quadriceps atrophy. These lead to significant functional impairment (limping, difficulty climbing stairs, reduced walking distance, and progressive inability to carry out daily activities).
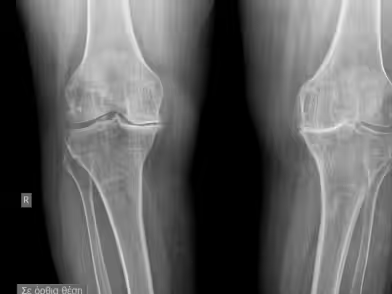

Plain X-rays of the knee, especially under load, are usually so characteristic that more specialized tests are often unnecessary. Typical findings include asymmetric narrowing of the joint space, sclerosis of the subchondral bone, osteophytes at the joint margins, and evidence of prior conditions (fractures, chondrocalcinosis, etc.)
CT and MRI can also confirm the presence of knee osteoarthritis, particularly in complex cases.
Stop living in pain, improve the quality of your life!
In the early stage, three actions involve the treatment of incipient osteoarthritis.
1) Analgesia (painkillers - non-steroidal anti-inflammatory drugs).
2) Mobilization (physiotherapy - kinesiotherapy).
3) Load reduction (weight loss, use of a cane, avoidance of unnecessary strain, periods of rest).
In the intermediate stage, if symptoms worsen, intra-articular injections may be used, including biological agents (PRP – stem cells), hyaluronic acid, as well as corrective osteotomies to realign the mechanical axis of the knee (in patients with stable joints and preserved mobility).
In the advanced stage, severe joint destruction with increased pain, instability, and deformity requires reconstructive surgery, namely total knee arthroplasty, which achieves excellent outcomes.
Multiple factors contribute to the pathogenesis of knee osteoarthritis: genetic predisposition, metabolic and hormonal influences on cartilage, degree of knee loading, local mechanical stresses, pre-existing arthritis, and traumatic cartilage injuries. These all result in reduced elasticity and diminished load-bearing capacity of the cartilage.
Knee osteoarthritis can be prevented to some extent by modifying these risk factors—such as weight reduction, physiotherapy, light exercise, swimming, and muscle strengthening.
to guide you about your condition, so you can choose the best possible treatment for it.
We use cookies to improve your experience on our site. By using our site, you consent to cookies.
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
These cookies are needed for adding comments on this website.
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Google Tag Manager simplifies the management of marketing tags on your website without code changes.
Marketing cookies are used to follow visitors to websites. The intention is to show ads that are relevant and engaging to the individual user.
Google Maps is a web mapping service providing satellite imagery, real-time navigation, and location-based information.
Service URL: policies.google.com (opens in a new window)