
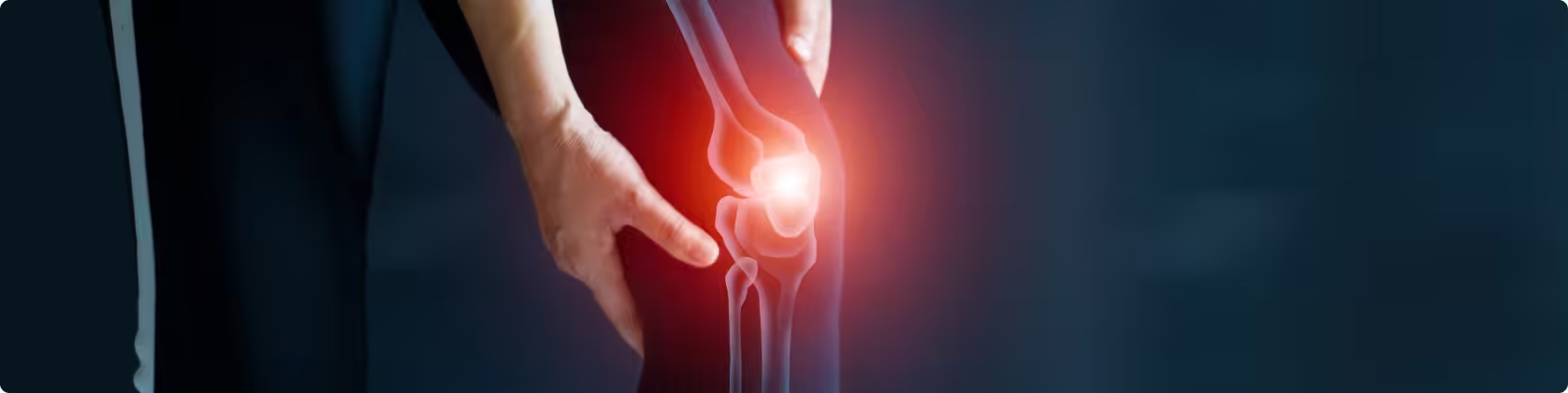
Cartilage is the smooth tissue covering the ends of bones within each joint. It is an important structure in the human body’s joints. There are three types of cartilage: elastic, fibrous, and hyaline, each with different locations and functions. Hyaline cartilage is the one that covers the joints.
Cartilage can sustain damage due to various factors, including injuries, inflammation, or degenerative conditions such as osteoarthritis.
Damage to articular cartilage may be referred to as a “chondral lesion” or “osteochondral lesion,” depending on whether only the cartilage is affected or the underlying bone tissue as well.
Knee cartilage lesions can result from sudden trauma, long-term joint overloading, degenerative conditions, or inflammation. They most commonly appear in younger or middle-aged individuals due to increased activity levels or the degenerative nature of joints.
Symptoms of a cartilage lesion may include pain, swelling, stiffness, and limited joint mobility. In more severe cases, patients may experience joint locking or instability.
Diagnosing knee cartilage lesions can be challenging since symptoms may resemble other conditions. Imaging methods such as X-rays, MRI, and arthroscopy are used to confirm the diagnosis.
Cartilage lesions are classified into five stages according to severity—from normal cartilage to complete loss of thickness with exposure of the underlying bone.
Importantly, the severity of a cartilage lesion does not always correlate with the degree of pain; rather, what matters is how the lesion affects joint movement, whether weight-bearing or not.
Stop living in pain, improve the quality of your life!
In the early stages, conservative treatment is preferable. It includes unloading the joint with crutches, cryotherapy, analgesics, anti-inflammatory drugs, avoidance of aggravating activities, and physiotherapy.
Intra-articular injections of PRP (platelet-rich plasma) or stem cells may provide temporary relief or even promote healing in cases of mild cartilage irritation. PRP primarily has anti-inflammatory effects, while hyaluronic acid reduces friction and enhances joint lubrication. Stem cells may offer regenerative potential, as they can differentiate into chondrocytes.
In advanced stages, surgery is necessary. Arthroscopy is the preferred method, allowing intervention through small incisions. Techniques include fixation, bone marrow stimulation with microfractures, osteochondral grafting, and scaffold implantation.
Autologous chondrocyte transplantation is a complex process in which cartilage cells are cultured and implanted into the lesion. Due to its cost and complexity, it is reserved for selected cases.
Artificial scaffolds are another advanced technique that attracts chondrocytes to develop new cartilage. Postoperative rehabilitation includes joint protection and gradual restoration of motion.
Microfracture technique (Microfractures)
This method has been used for more than 30 years in orthopedic cartilage repair. With specialized arthroscopic tools, the bone marrow beneath the subchondral bone is stimulated, releasing stem cells to fill the cartilage defect. These cells then differentiate into about 70–75% cartilage cells and 25–30% fibrous cells.
Success rates reach 90–95% for lesions smaller than 1 cm³. Younger, non-smoking, non-diabetic patients show the best outcomes..
Autologous osteochondral transplantation (OATS)
For larger lesions (>1 cm³), especially in weight-bearing areas, autologous osteochondral grafts can be harvested from non-weight-bearing zones and transplanted. Postoperative care includes 4 weeks of unloading and progressive loading over 2.5–3 months.
The success rate of this knee surgery internationally reaches 85 to 90%, similar to our results of 90 to 95%. The younger the age of the patient ("rich" in cartilage cells, the autograft and the neovascularization develop faster due to the "rich" bone marrow), as well as in non-smokers or non-sugar diabetics, the better results we observe.
Autologous Cancellous Bone with Periosteum
This method, developed in Hungary in the 1990s, is used for extensive knee cartilage lesions (>1.5 cm³) or difficult anatomical sites such as the femoral condyles. Necrotic bone is removed, cancellous bone graft is harvested from the tibia or iliac crest, and a periosteal flap is sutured over the lesion. Success rates are 85–90%.
Allograft Cartilage Transplantation
If a knee cartilage lesion is too large for an autograft, an allograft may be used. Donor tissue from cadavers includes both cartilage and bone, often in large sizes (even an entire femoral condyle). After sterilization and screening for infectious diseases, the graft is prepared.
However, sterilization and irradiation reduce cell numbers, lowering success rates compared to autografts.
With proper physiotherapy and a structured rehabilitation program, most patients can return to daily activities within 4 to 9 months after surgery.
Cartilage is the smooth tissue covering the ends of bones within each joint. It is an important structure in the human body’s joints. There are three types of cartilage: elastic, fibrous, and hyaline, each with different locations and functions. Hyaline cartilage is the one that covers the joints.
Cartilage can sustain damage due to various factors, including injuries, inflammation, or degenerative conditions such as osteoarthritis.
Damage to articular cartilage may be referred to as a “chondral lesion” or “osteochondral lesion,” depending on whether only the cartilage is affected or the underlying bone tissue as well.
Knee cartilage lesions can result from sudden trauma, long-term joint overloading, degenerative conditions, or inflammation. They most commonly appear in younger or middle-aged individuals due to increased activity levels or the degenerative nature of joints.
Symptoms of a cartilage lesion may include pain, swelling, stiffness, and limited joint mobility. In more severe cases, patients may experience joint locking or instability.
Diagnosing knee cartilage lesions can be challenging since symptoms may resemble other conditions. Imaging methods such as X-rays, MRI, and arthroscopy are used to confirm the diagnosis.
Cartilage lesions are classified into five stages according to severity—from normal cartilage to complete loss of thickness with exposure of the underlying bone.
Importantly, the severity of a cartilage lesion does not always correlate with the degree of pain; rather, what matters is how the lesion affects joint movement, whether weight-bearing or not.
In the early stages, conservative treatment is preferable. It includes unloading the joint with crutches, cryotherapy, analgesics, anti-inflammatory drugs, avoidance of aggravating activities, and physiotherapy.
Intra-articular injections of PRP (platelet-rich plasma) or stem cells may provide temporary relief or even promote healing in cases of mild cartilage irritation. PRP primarily has anti-inflammatory effects, while hyaluronic acid reduces friction and enhances joint lubrication. Stem cells may offer regenerative potential, as they can differentiate into chondrocytes.
In advanced stages, surgery is necessary. Arthroscopy is the preferred method, allowing intervention through small incisions. Techniques include fixation, bone marrow stimulation with microfractures, osteochondral grafting, and scaffold implantation.
Autologous chondrocyte transplantation is a complex process in which cartilage cells are cultured and implanted into the lesion. Due to its cost and complexity, it is reserved for selected cases.
Artificial scaffolds are another advanced technique that attracts chondrocytes to develop new cartilage. Postoperative rehabilitation includes joint protection and gradual restoration of motion.
Microfracture technique (Microfractures)
This method has been used for more than 30 years in orthopedic cartilage repair. With specialized arthroscopic tools, the bone marrow beneath the subchondral bone is stimulated, releasing stem cells to fill the cartilage defect. These cells then differentiate into about 70–75% cartilage cells and 25–30% fibrous cells.
Success rates reach 90–95% for lesions smaller than 1 cm³. Younger, non-smoking, non-diabetic patients show the best outcomes..
Autologous osteochondral transplantation (OATS)
For larger lesions (>1 cm³), especially in weight-bearing areas, autologous osteochondral grafts can be harvested from non-weight-bearing zones and transplanted. Postoperative care includes 4 weeks of unloading and progressive loading over 2.5–3 months.
The success rate of this knee surgery internationally reaches 85 to 90%, similar to our results of 90 to 95%. The younger the age of the patient ("rich" in cartilage cells, the autograft and the neovascularization develop faster due to the "rich" bone marrow), as well as in non-smokers or non-sugar diabetics, the better results we observe.
Autologous Cancellous Bone with Periosteum
This method, developed in Hungary in the 1990s, is used for extensive knee cartilage lesions (>1.5 cm³) or difficult anatomical sites such as the femoral condyles. Necrotic bone is removed, cancellous bone graft is harvested from the tibia or iliac crest, and a periosteal flap is sutured over the lesion. Success rates are 85–90%.
Allograft Cartilage Transplantation
If a knee cartilage lesion is too large for an autograft, an allograft may be used. Donor tissue from cadavers includes both cartilage and bone, often in large sizes (even an entire femoral condyle). After sterilization and screening for infectious diseases, the graft is prepared.
However, sterilization and irradiation reduce cell numbers, lowering success rates compared to autografts.
With proper physiotherapy and a structured rehabilitation program, most patients can return to daily activities within 4 to 9 months after surgery.
to guide you about your condition, so you can choose the best possible treatment for it.
We use cookies to improve your experience on our site. By using our site, you consent to cookies.
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
These cookies are needed for adding comments on this website.
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Google Tag Manager simplifies the management of marketing tags on your website without code changes.
Marketing cookies are used to follow visitors to websites. The intention is to show ads that are relevant and engaging to the individual user.
Google Maps is a web mapping service providing satellite imagery, real-time navigation, and location-based information.
Service URL: policies.google.com (opens in a new window)